Chelation
What is chelation and how can it help improve autism symptoms?
Heavy metals and aluminium have are often found in high levels within the body and brains of children with autism.
Chelation or chelation therpy is a method of helping the body clear these metals by binding to them and making them easier to clear by the kidneys or liver.
The chemicals used in chelation are designed to bind to metals and aluminium depending on the type used.
However, there if used inappropriately there is risk of harm such as low calcium levels, extraction of essential metals from the body such as zinc or copper, kidney failure and liver problems.
We recommend just like all interventions on this website you consult your doctor including chelation.
If you are unsure wheather metals or aluminium are affecting your child or possibly contributing to autism symptoms then speak to your doctor about blood tests to measure levels like mercury, lead, cadnium and aluminium.
If you doctor is not comfortble with helping then find one who will.
SPEAK TO YOUR DOCTOR ABOUT CHELATION.
CHELATION CLEARS OUT TOXIN METALS IN THE BODY BUT CAN ALSO CLEAR OUT MINERNALS YOU NEED.
LOW CALCIUM, ZINC, MAGNESIUM AND COPPER CAN BE OCCUR AND CAN EVEN LEAD TO SERIOUS HARM OR DEATH.
IT HAS BEEN SHOWN TO HELP MANY CHILDREN WITH AUTISM, BUT THERE HAS BEEN REPORTS OF DEATH FROM PARTICULAR CHELATION THERAPY WHICH WAS GIVEN INCORRECTLY IN HOSPITAL.



Chelation therapy can include chemicals like such as:
DSMA (dimercaptosuccinic acid)
EDTA ( Ethylenediaminetetraacetic acid)
Dimercaprol
Penicillamine
Some are given IV and others orally.


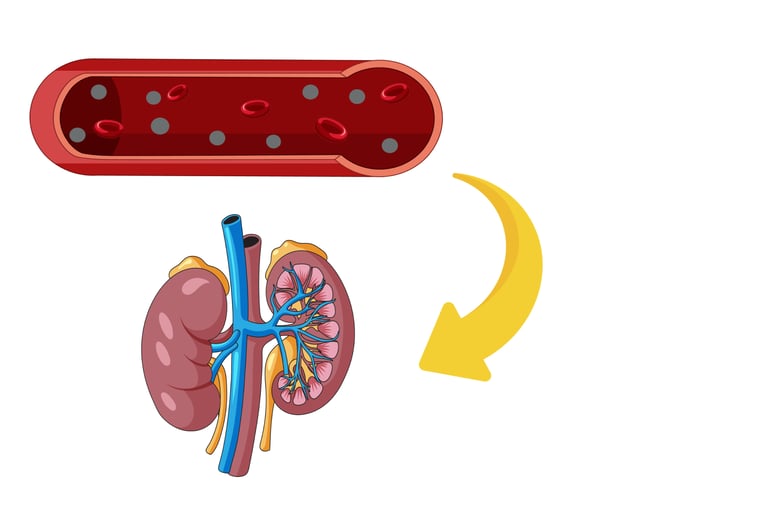
Heavy metals or aluminium in the body causing harm and disrupting development.
Chelators bind to these heavy metals and aluminium.
They make it easier for the liver and kidneys to clear it from the body typically via urine or fecaes.
It then leaves the body with studies showing it has helped improve autism symptoms such as....
How chelation works
How to used chelation therapy
Pros
Behavioral Benefits: DMSA therapy, especially the 7-round treatment, was associated with significant improvements in behavioral symptoms of autism across multiple assessment tools (ATEC, PDD-BI, SAS, ADOS, PGI).
Biological Correlation: Improvements in the 7-round group were strongly linked to the excretion of toxic metals and changes in glutathione levels, providing evidence of a biological mechanism rather than a placebo effect.
Safety Profile: The therapy was generally safe, with no significant adverse effects on gut function or other areas, except for a slight, often temporary increase in hyperactivity in some cases. DMSA is also FDA-approved for lead poisoning, supporting its established safety record.
Age Inclusivity: Benefits were observed across a range of ages, making it potentially applicable to both younger and older children with ASD.
Cons
Study Design Limitations: The study was not a true placebo-controlled trial because the initial screening round in Phase 1 affected glutathione and platelet levels, potentially influencing subsequent results and complicating interpretation.
Unclear Dosage and Duration: The exact dose and total treatment duration are not specified in this document, limiting the ability to replicate or apply the findings clinically without additional information.
Mixed Outcomes: Approximately 11% of participants experienced a slight worsening of symptoms, and some showed temporary hyperactivity, indicating that the therapy may not benefit all children equally.
Limited Additional Benefit: The 7-round group did not show significantly greater improvements than the 1-round group, raising questions about the necessity or added value of multiple rounds.
Need for Further Research: Longer-term studies are required to assess whether extended treatment yields greater benefits and to confirm the findings in a more controlled setting
[CH 1]
Pros
Behavioral Gains: Significant reductions in autism severity, particularly in sociability, cognitive awareness, and behavior, as measured by ATEC.
Hyperandrogenemia Relief: Effective reduction of symptoms like early puberty and aggression.
Safety: Minimal impact on essential minerals and organ function; prior studies suggest Lupron is safe long-term for reproductive health.
Biological Effects: Confirmed reductions in androgen levels and increased heavy metal excretion, supporting the treatment’s mechanism.
Quick Response: Some improvements observed within days of starting Lupron.
Cons
Small Sample Size: Only 11 children, limiting the ability to generalize findings.
No Control Group: The open-label design raises questions about whether improvements were due to the treatment or other factors (e.g., placebo effect).
Side Effects: Gastrointestinal disturbances in some cases, though manageable with transdermal DMSA.
Unknown Long-Term Effects: While short-term safety was shown, long-term impacts (e.g., on reproduction) remain unstudied in this context.
Complexity: Multiple medications and administration routes may pose logistical challenges for families.
[CH 2]
Pros
Comprehensive Approach: The treatment addressed multiple factors (nutrition, environment, chelation, and therapies), potentially offering a holistic benefit.
Significant Improvements: All 10 children showed progress in behavior, social skills, and academic abilities, with some returning to regular classrooms.
Reduction in Heavy Metal Burden: The significant drop in urinary lead levels suggests effective detoxification, which may correlate with clinical improvements.
Cons
Small Sample Size: Only 10 patients were included, limiting the generalizability of the findings.
Lack of Control Group: Without a control group, it’s unclear whether improvements were due to the treatment, ongoing therapies, or natural development.
Not Randomized or Blinded: The open-label design increases the risk of bias from parents, teachers, or clinicians.
Lack of Specific Details: The absence of exact chelator doses and precise timelines for symptom improvement hinders replication and interpretation.
Multifaceted Treatment: The use of multiple interventions simultaneously makes it difficult to determine which component (e.g., chelation, nutrition, or therapy) drove the observed effects.
[CH 3]